Sleep-Wake Disturbances

More than 50% of patients report sleep disturbances following concussion, specifically insomnia, hypersomnia, obstructive sleep apnea, poor sleep maintenance, poor sleep efficiency, early awakening, delayed sleep onset, or alterations in circadian cycle. (see Appendix 7.1).1-5 In the immediate acute stage of concussion, there may be an increased need for sleep6, however, this decreases over time and insomnia is the most common form of sleep disturbance reported in the subacute and chronic stages of concussion.
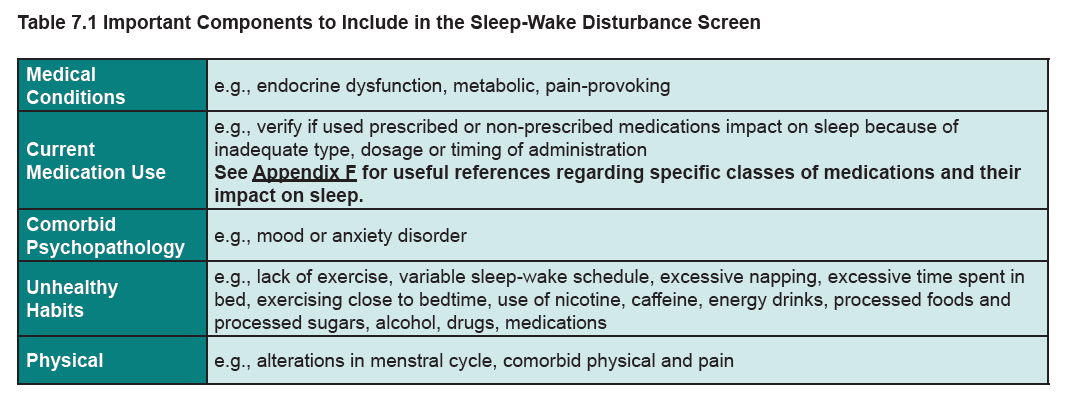
Obtaining a history from the patient to record the concussion, to rule out pre-existing sleep disorders, and to document symptoms after the injury is key. Once a thorough evaluation has been conducted, treatment of sleep disorders within the concussion population may take the form of both non-pharmacologic and pharmacologic methods. For insomnia, cognitive behavioural therapy (CBT) is recommended7-9. Referral to a professional with training and expertise in CBT for insomnia is ideal, however, while waiting for formalized CBT treatment for insomnia, or if this treatment is not available, behavioral recommendations (e.g., restriction of time in bed and stimulus control) can still be implemented by primary care providers2,8,10. Referral to a sleep specialist is essential to evaluate and treat less common sleep problems associated with concussion, such as a sleep-related breathing disorder (e.g., obstructive sleep apnea), circadian rhythm shift, restless leg syndrome, periodic limb movement disorder, and REM sleep behaviour disorder.
References supporting introduction:
- Mathias JL, Alvaro PK. Prevalence of sleep disturbances, disorders, and problems following traumatic brain injury: a meta- analysis. Sleep Med. 2012;13(7):898-905.
- Baumann CR. Traumatic brain injury and disturbed sleep and wakefulness. Neuromolecular Med. 2012;14(3):205-212.
- Wiseman-Hakes C, Colantonio A, Gargaro J. Sleep and wake disorders following traumatic brain injury: A systematic review of the literature. Critical Reviews in Physical and Rehabilitation Medicine. 2009;21(3-4):317-374.
- Castriotta RJ, Wilde MC, Lai JM, Atanasov S, Masel BE, Kuna ST. Prevalence and consequences of sleep disorders in traumatic brain injury. J Clin Sleep Med. 2007;3(4):349-356.
- Theadom A, Cropley M, Parmar P, et al. Sleep difficulties one year following mild traumatic brain injury in a population-based study. Sleep Med. 2015;16(8):926-932.
- Raikes AC, Schaefer SY. Sleep Quantity and Quality during Acute Concussion: A Pilot Study. Sleep. 2016;39(12):2141-2147.
- Ouellet MC, Morin CM. Efficacy of cognitive-behavioral therapy for insomnia associated with traumatic brain injury: a single case experimental design. Arch Phys Med Rehabil. 2007;88(12):1581-1592.
- Ouellet MC, Morin CM. Cognitive behavioral therapy for insomnia associated with traumatic brain injury: a single-case study. Arch Phys Med Rehabil. 2004;85(8):1298-1302 23.
- Espie CA, MacMahon KM, Kelly HL, et al. Randomized clinical effectiveness trial of nurse-administered small-group cognitive behavior therapy for persistent insomnia in general practice. Sleep. 2007;30(5):574-584.
- Castriotta RJ, Murthy JN. Sleep disorders in patients with traumatic brain injury: a review. CNS Drugs. 2011;25(3):175-185.
Patients should be routinely screened for sleep-related problems (i.e., sleep disturbances). For those screening positive, sleep should be evaluated using a validated assessment tool; particularly for insomnia.
Insomnia is a prevalent sleep-wake disorder following concussion, with symptoms present in roughly 70% of patients. Older patients and those of female gender are at increased risk for disturbances in the sleep-wake cycle. Those patients presenting with significant sleep disturbances should be screened for insomnia using a validated tool, such as the Insomnia Severity Index in order to guide treatment planning. If other sleep disorders are suspected, sleep quality may be assessed using the Pittsburgh Sleep Quality Index.
References supporting context:
- Montgomery, M. C., Baylan, S., & Gardani, M. Prevalence of insomnia and insomnia symptoms following mild-traumatic brain injury: A systematic review and meta-analysis. Sleep medicine reviews. 2022;61, 101563.
- Oyegbile, T. O., Delasobera, B. E., & Zecavati, N. Gender differences in sleep symptoms after repeat concussions. Sleep medicine. 2017;40, 110–115.
- Wei, L., Wen, Y. T., Thompson, H. J., Liu, C. Y., Su, Y. K., Chen, P. Y., Chen, C. Y., Chuang, Y. H., Lin, Y. J., Chen, C. T., Chen, C. C., Chiu, H. T., & Chiu, H. Y. Sleep Disturbances Following Traumatic Brain Injury in Older Adults: A Comparison Study. The Journal of head trauma rehabilitation. 2020;35(4), 288–295.
- Wickwire, E. M., Albrecht, J. S., Capaldi, V. F., 2nd, Jain, S. O., Gardner, R. C., Werner, J. K., Mukherjee, P., McKeon, A. B., Smith, M. T., Giacino, J. T., Nelson, L. D., Williams, S. G., Collen, J., Sun, X., Schnyer, D. M., Markowitz, A. J., Manley, G. T., Krystal, A. D., & Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) Investigators. Trajectories of Insomnia in Adults After Traumatic Brain Injury. JAMA network open. 2022;5(1), e2145310.
- Wiseman-Hakes, C., Foster, E., Langer, L., Chandra, T., Bayley, M., & Comper, P. Characterizing Sleep and Wakefulness in the Acute Phase of Concussion in the General Population: A Naturalistic Cohort from the Toronto Concussion Study. Journal of neurotrauma. 2022;39(1-2), 172–180.
Patient education and treatment of sleep disturbances should be prioritized (along with headache and mood), given their significant impact and interaction with other functionally limiting symptoms including:
- Pain
- Fatigue
- Mood disturbances
- Cognitive problems
Patients and their support person should be educated using written, verbal and/or pictorial formats.
Patients should be reassured that sleep-wake disorders are common following concussion, and most patients have mild symptoms and achieve full recovery with time. Patients should be informed that most sleep related problems will resolve spontaneously; however, targeted intervention may be required to facilitate recovery. Patients should be made aware that poor sleep may exacerbate other symptoms such as headache, fatigue, mood disturbances and cognitive problems possibly contributing to delayed recovery. This interaction may be referred to as the vicious cycle of symptoms. Targeted treatment of sleep disturbances, alongside other more disabling symptoms of headache, fatigue and mood is likely to improve overall recovery.
References supporting context:
- Montgomery, M. C., Baylan, S., & Gardani, M. Prevalence of insomnia and insomnia symptoms following mild-traumatic brain injury: A systematic review and meta-analysis. Sleep medicine reviews. 2022;61, 101563.
- Kalmbach, D. A., Conroy, D. A., Falk, H., Rao, V., Roy, D., Peters, M. E., Van Meter, T. E., & Korley, F. K. (2018). Poor sleep is linked to impeded recovery from traumatic brain injury. Sleep, 41(10), zsy147.
- Wickwire, E. M., Albrecht, J. S., Capaldi, V. F., 2nd, Jain, S. O., Gardner, R. C., Werner, J. K., Mukherjee, P., McKeon, A. B., Smith, M. T., Giacino, J. T., Nelson, L. D., Williams, S. G., Collen, J., Sun, X., Schnyer, D. M., Markowitz, A. J., Manley, G. T., Krystal, A. D., & Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) Investigators. Trajectories of Insomnia in Adults After Traumatic Brain Injury. JAMA network open. 2022;5(1), e2145310.
- Wickwire, E. M., Schnyer, D. M., Germain, A., Williams, S. G., Lettieri, C. J., McKeon, A. B., Scharf, S. M., Stocker, R., Albrecht, J., Badjatia, N., Markowitz, A. J., & Manley, G. T. (2018). Sleep, Sleep Disorders, and Circadian Health following Mild Traumatic Brain Injury in Adults: Review and Research Agenda. Journal of neurotrauma, 35(22), 2615–2631.
( Education )
( Interaction with other symptoms )
Patients with insomnia should be referred for cognitive behavioural therapy (CBT) specifically for sleep. If CBT is not easily accessible, the primary care provider should minimally provide information for sleep hygiene and self-management strategies or programs.
CBT is established as the treatment of choice for sleep-wake disorders following concussion. If CBT provided by a licensed practitioner is not available, remote delivery of CBT and self-management strategies are also effective to reduce sleep wake disturbances. CBT for persistent insomnia should incorporate:
-
Sleep restriction: limiting time spent in bed during the day
-
Stimulus control: build associations between the bedroom and sleep
-
Relaxation: e.g., deep breathing, progressive muscular relaxation
-
Cognitive therapy: address thoughts, beliefs, and attitudes related to sleep and consequences of sleep problems
-
Meditation
For virtual CBT resources, please view the following: CBT-I coach, Sleep Foundation.
References supporting context:
- Sullivan, K. A., Blaine, H., Kaye, S. A., Theadom, A., Haden, C., & Smith, S. S. A Systematic Review of Psychological Interventions for Sleep and Fatigue after Mild Traumatic Brain Injury. Journal of neurotrauma. 2018;35(2), 195–209.
- Theadom, A., Barker-Collo, S., Jones, K., Dudley, M., Vincent, N., & Feigin, V. A pilot randomized controlled trial of on-line interventions to improve sleep quality in adults after mild or moderate traumatic brain injury. Clinical rehabilitation. 2018;32(5), 619–629.
( CBT )
( Sleep hygiene and self-management )
Other non-pharmacologic treatment options that have been found to be useful in the treatment of insomnia include:
-
Melatonin (taken 2 hours before bedtime in conjunction with reduced evening light exposure and blue light therapy in the morning)
-
Magnesium and zinc supplementation
-
Acupuncture
-
Mindfulness-based stress reduction therapy
Several supplements have been found useful to promote sleep. Melatonin is a natural hormone supplement that is used to adjust the body's internal clock, or circadian rhythm. Taking 2-5mg 2 hours before bedtime can help restore sleep and improve daytime alertness in patients following brain injury. Magnesium can make you feel drowsy, which can help you fall asleep. It may also reduce the frequency of migraine headaches. The most common side effect is diarrhea which is dose-dependent. Start at a low dose and gradually work your way up as tolerated. Between 200-400mg at bedtime is recommended. Certain foods also contain magnesium, such as legumes, nuts, whole grains, seeds, green leafy vegetables, soy products, bananas, and avocados. Additionally, dietary zinc has been shown to help increase the amount of quality sleep. Primary care providers may recommend 10-20mg of zinc at bedtime. Foods containing zinc include lean red meats, seafood, peas, and beans.
( Blue light )
( Acupuncture )
( Remaining )
If non-pharmacological treatment options have not been effective for the patient, medications could be considered to facilitate sleep. The following principles must be considered:
-
Avoid medications that may lead to dependency
-
Aim for a short duration of use
-
Recognize potential adverse effects and medication interactions
-
Prescribe medications which may manage multiple co-occurring symptoms
-
Avoid polypharmacy
-
Start at a low dose and gradually increase as tolerated
Pharmacological treatment options can be used to establish a more routine sleep-wake pattern using agents with minimal risk of dependency and adverse effects in patients with concussion. Medications to be considered include low-dose trazodone and tricyclic antidepressants (e.g., Amitryptyline, Doxepine), as well as mirtazapine. Prazosin may be considered in patients with nightmares and PTSD. Benzodiazepines should generally be avoided; however, nonbenzodiazepine medications (e.g., Zopiclone, Exzopiclone) may have fewer adverse effects and may be considered for short-term use.
References supporting context:
- Reprinted with Permission from Centre for Effective Practice. (January 2017). Management of Chronic Insomnia: Ontario. Toronto: Centre for Effective Practice.
When criteria are met for chronic insomnia, sleep should be monitored for improvement over time using validated patient-reported outcome measures or sleep monitoring devices.
Other sleep-wake disturbances and medical conditions that influence sleep should be screened for, treated, and monitored.
To monitor and improve sleep habits, patients may benefit from sleep monitoring devices such as a sleep diary, or technological solutions for monitoring sleep (e.g., smart watches). These devices may aid in accurately monitoring and assessing the efficacy of current treatments in relation to the number of hours of sleep per night, the number of times one wakes up throughout the night, antecedents, and disturbances which may be impacting sleep.
References supporting context:
- Morse, A. M., & Kothare, S. V. (2018). Sleep disorders and concussion. Handbook of clinical neurology, 158, 127–134.
Referral for a sleep specialist consultation and/or sleep study should be considered if insomnia and/or excessive daytime sleepiness persists or there is suspicion of other sleep-related disorders.
Referral should be considered if there is suspicion of nocturnal seizures, insomnia disorder, circadian rhythm sleep disorder, sleep-related breathing disorders, sleep-related movement disorders, sleep apnea, parasomnia, or hypersomnia.
EVALUATION
Title of Resource: Short Clinical Interview for Sleep after Head Injury
Reference: Ouellet MC, Beaulieu-Bonneau S Morin CM. Sleep-Wake Disturbances. In Eds. Zasler ND, Katz DI, Zafonte RD. Brain Injury Medicine: Principles and Practice. New York; Demos Medical Publishing LLC; 2012.
Description: The short clinical interview for sleep after head injury was designed to qualitatively assess for common sleep or sleep/wake disturbances and changes after brain injury as well as a history of the problem.
Resource Criteria:
PopulationAdults with Head Injury
Reliability/ Validity
NA
Proprietary?
Yes
Time to Administer
6-15 minutes
Method to Administer
Patient Interview
Formal Instructions (Mention if special environment/ equipment is needed)
NA
Instructional Video Available?
No
Ease of Use (By Patient)
Very Difficult 1 2 3 4 5 Very Easy
Ease of Administration (By Administrator)
Very Difficult 1 2 3 4 5 Very Easy
Other Comments
None
EVALUATION
Title of Resource: Sleep and Concussion Questionnaire
Reference: Catherine Wiseman-Hakes & Marie-Christine Ouellet (Expert Consensus Members)
Description: 5-item self-report questionnaire used to determine severity of changes in sleep/wake patterns after a mild TBI/concussion.
Resource Criteria:
Population
Post-concussion sleep problems
Reliability/ Validity
The reliability/validity of the Sleep & Concussion Questionnaire is not yet available.
Proprietary?
No
Time to Administer
5 minutes
Method to Administer
Self-report questionnaire
Formal Instructions (Mention if special environment/ equipment is needed)
None
Instructional Video Available?
No
Ease of Use (By Patient)
Very Difficult 1 2 3 4 5 Very Easy
Ease of Administration (By Administrator)
Very Difficult 1 2 3 4 5 Very Easy
Other Comments
None
{kind=link}
Zalai, D. M., Girard, T. A., Cusimano, M. D., & Shapiro, C. M. Circadian rhythm in the assessment of postconcussion insomnia: a cross-sectional observational study. CMAJ open. 2020;8(1), E142–E147.
STROBE: 20/23
Associated with recommendation 7.1
Toccalino D, Wiseman-Hakes C, Zalai DM. Preliminary Validation of the Sleep and Concussion Questionnaire as an Outcome Measure for Sleep Following Brain Injury. Brain Inj. 2021;35(7):743-750.
STROBE: 18/23
Associated with recommendation 7.1
Chan LG, Feinstein A. Persistent Sleep Disturbances Independently Predict Poorer Functional and Social Outcomes 1 Year After Mild Traumatic Brain Injury. J Head Trauma Rehabil. 2015;30(6):E67-75.
DOWNS & BLACK: 13/32
Associated with recommendation 7.2 (interaction with other symptoms)
Kalmbach, D. A., Conroy, D. A., Falk, H., Rao, V., Roy, D., Peters, M. E., Van Meter, T. E., & Korley, F. K. Poor sleep is linked to impeded recovery from traumatic brain injury. Sleep. 2018;41(10), zsy147.
STROBE: 17/23
Associated with recommendation 7.2 (interaction with other symptoms)
Mollayeva, T., Sharma, B., Vernich, L., Mantis, S., Lewko, J., Gibson, B., Liss, G., Kontos, P., Grigorovich, A., & Colantonio, A. Sleep before and after work-related concussion: Sex differences in effects and functional outcomes. Work (Reading, Mass.). 2020;67(4), 927–938.
STROBE: 17/23
Associated with recommendation 7.2 (interaction with other symptoms)
Oyegbile, T. O., Delasobera, B. E., & Zecavati, N. Gender differences in sleep symptoms after repeat concussions. Sleep medicine. 2017;40, 110–115.
STROBE: 16/23
Associated with recommendation 7.2 (interaction with other symptoms)
Sullan, M. J., Crocker, L. D., Thomas, K. R., Orff, H. J., Davey, D. K., Jurick, S. M., Twamley, E. W., Norman, S. B., Schiehser, D. M., Aupperle, R., & Jak, A. J. Baseline sleep quality moderates symptom improvement in veterans with comorbid PTSD and TBI receiving trauma-focused treatment. Behaviour research and therapy. 2021;143, 103892.
Downs & Black: 22/28
Associated with recommendation 7.2 (interaction with other symptoms)
Theadom A, Cropley M, Parmar P, et al. Sleep difficulties one year following mild traumatic brain injury in a population-based study. Sleep Med. 2015;16(8):926-932.
DOWNS & BLACK: 16/32
Associated with recommendation 7.2 (interaction with other symptoms)
Tkachenko N, Singh K, Hasanaj L, Serrano L, Kothare SV. Sleep Disorders Associated With Mild Traumatic Brain Injury Using Sport Concussion Assessment Tool 3. Pediatr Neurol. 2016;57:46-50.e41.
DOWNS & BLACK: 12/32
Associated with recommendation 7.2 (interaction with other symptoms)
Wiseman-Hakes, C., Foster, E., Langer, L., Chandra, T., Bayley, M., & Comper, P. Characterizing Sleep and Wakefulness in the Acute Phase of Concussion in the General Population: A Naturalistic Cohort from the Toronto Concussion Study. Journal of neurotrauma. 2022;39(1-2), 172–180.
STROBE: 17/23
Associated with recommendation 7.2 (interaction with other symptoms)
Kraemer Y, Mäki K, Marinkovic I, et al. Post-traumatic headache after mild traumatic brain injury in a one-year follow up study - risk factors and return to work. J Headache Pain. 2022;23(1):27.
STROBE: 18/23
Associated with recommendation 7.2 (interaction with other symptoms)
Hromas GA, Houck ZM, Asken BM, et al. Making a Difference: Affective Distress Explains Discrepancy Between Objective and Subjective Cognitive Functioning After Mild Traumatic Brain Injury. J Head Trauma Rehabil. 2021;36(3):186-195.
STROBE: 19/23
Associated with recommendation 7.2 (interaction with other symptoms)
Rakers SE, Timmerman ME, Scheenen ME, et al. Trajectories of Fatigue, Psychological Distress, and Coping Styles After Mild Traumatic Brain Injury: A 6-Month Prospective Cohort Study. Arch Phys Med Rehabil. 2021;102(10):1965-1971.e2.
STROBE: 20/23
Associated with recommendation 7.2 (interaction with other symptoms)
Skandsen T, Stenberg J, Follestad T, et al. Personal Factors Associated With Postconcussion Symptoms 3 Months After Mild Traumatic Brain Injury. Arch Phys Med Rehabil. 2021;102(6):1102-1112.
STROBE: 21/23
Associated with recommendation 7.2 (interaction with other symptoms)
Anderson JFI, Jordan AS. An observational study of the association between sleep disturbance, fatigue and cognition in the post-acute period after mild traumatic brain injury in prospectively studied premorbidly healthy adults. Neuropsychol Rehabil. 2021;31(9):1444-1465.
STROBE: 19/23
Associated with recommendation 7.2 (interaction with other symptoms)
Brett BL, Meier TB, Savitz J, Guskiewicz KM, McCrea MA. Research Letter: Sleep Mediates the Association Between Prior Concussion and Depressive Symptoms. J Head Trauma Rehabil. 2021;36(4):E284-E288.
STROBE: 18/23
Associated with recommendation 7.2 (interaction with other symptoms)
Theadom, A., Barker-Collo, S., Jones, K., Dudley, M., Vincent, N., & Feigin, V. A pilot randomized controlled trial of on-line interventions to improve sleep quality in adults after mild or moderate traumatic brain injury. Clinical rehabilitation. 2018;32(5), 619–629.
Downs & Black: 15/28
Associated with recommendation 7.3 (CBT)
Sullivan KA, Blaine H, Kaye SA, Theadom A, Haden C, Smith SS. A Systematic Review of Psychological Interventions for Sleep and Fatigue after Mild Traumatic Brain Injury. J Neurotrauma. 2018;35(2):195-209.
AMSTAR 2: 14/20
Associated with recommendation 7.3 (CBT)
Srisurapanont K, Samakarn Y, Kamklong B, et al. Blue-wavelength light therapy for post-traumatic brain injury sleepiness, sleep disturbance, depression, and fatigue: A systematic review and network meta-analysis. PLoS One. 2021;16(2):e0246172.
AMSTAR 2: 16/20
Associated with recommendation 7.4 (blue light)
Bajaj S, Vanuk JR, Smith R, Dailey NS, Killgore WDS. Blue-Light Therapy following Mild Traumatic Brain Injury: Effects on White Matter Water Diffusion in the Brain. Front Neurol. 2017;8:616.
Downs & Black: 15/28
Associated with recommendation 7.4 (blue light)
Raikes AC, Dailey NS, Forbeck B, Alkozei A, Killgore WDS. Daily Morning Blue Light Therapy for Post-mTBI Sleep Disruption: Effects on Brain Structure and Function. Front Neurol. 2021;12:625431.
Downs & Black: 19/28
Associated with recommendation 7.4 (blue light)
Huang W, Johnson TM, Kutner NG, et al. Acupuncture for Treatment of Persistent Disturbed Sleep: A Randomized Clinical Trial in Veterans With Mild Traumatic Brain Injury and Posttraumatic Stress Disorder. J Clin Psychiatry. 2018;80(1):18m12235.
Downs & Black: 26/28
Associated with recommendation 7.4 (acupuncture)