Mental Health Disorders

Mental health symptoms and outcomes must be understood within the biopsychosocial context of the individual and consider that multiple factors can influence related mental health disorders. In the case of concussion, biologically the individual may suffer an insult to the brain and injuries to the body (e.g., whiplash injuries, etc.), with consequences to their experience of pain and ability to sleep, which can further cause changes in the neurobiology of the brain. At the psychological level they may experience acute stress due to their experience of trauma or injury, as well as in response to the consequences of their functional abilities resulting from the injury. People with persistent symptoms may become isolated from others as they may be intolerant of or unable to engage in social interactions. Their injury status may disrupt their occupational status, leisure activities and interpersonal interactions. They may also incur losses (e.g., reduced quality of life and independence; lowered income or reduced educational attainment; changes in relationship functioning, etc.). When assessing and managing disorders of mental health post concussion, it is important to consider all of these potential factors; additionally, individuals who have suffered a concussion may also have a pre-existing history of biopsychosocial factors/issues that may affect the expression of mental health symptoms or the duration of recovery including the ability to return to pre-injury status.
Screening for mental health symptoms early on and determining their etiology as well as prescribing treatment is crucial to facilitating a positive recovery. For example, in a primary care setting this may include screening for disturbances of sleep, or presence of chronic pain, loss, metabolic status etc when patients report low affect. Intervening at the level of improving sleep, managing pain and correcting metabolic imbalances may result in improving reports of low affect.
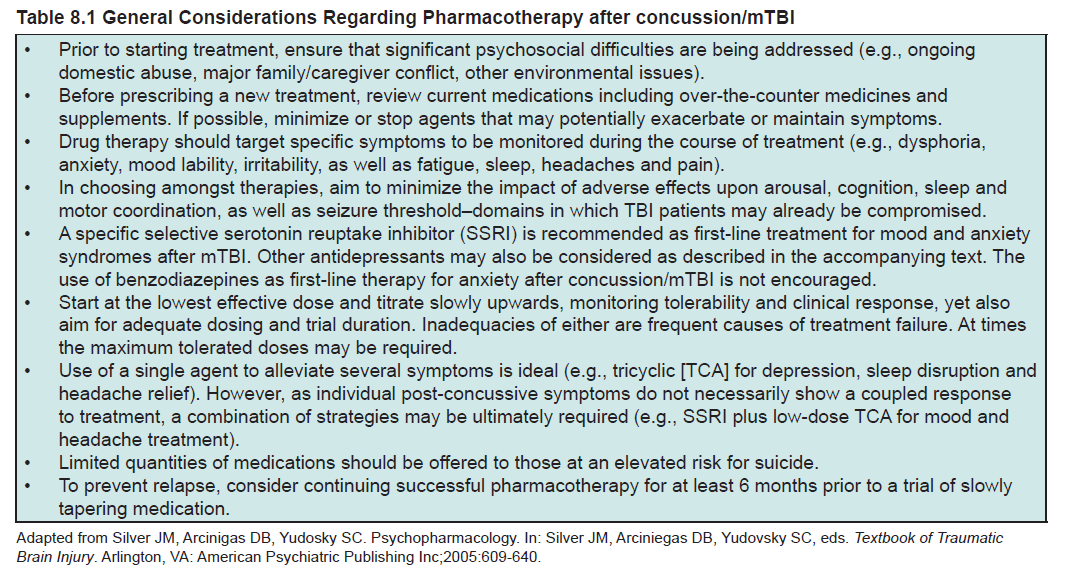
There is no current evidence to indicate that the mental health problems of individuals who have suffered a concussion should be treated any differently than mental health problems of other etiologies. As such, pharmacological and nonpharmacological interventions including therapeutic interventions that have been found to be helpful in the general population should be considered for individuals who have developed mental health problems post concussion. Strategies used to treat mental health symptoms post concussion/concussion should follow the same logic as that applied to similar symptoms found secondary to their conditions or circumstances which include the potential for treatments to worsen other concussion outcomes. For example, some antidepressant medications, particularly those that are more sedating and/or have greater anticholinergic activity, can worsen the anergia and cognitive impairments that arise directly from concussion. In general, psychotropic medications should be used with caution, and non-medication options selected as much as possible. If selecting a medication intervention, start at low doses, allow adequate time for response to be assessed for, and carefully monitor for both efficacy and side effects.
( Sleep )
( Pain )
( Remaining )
( Depression )
( Anxiety )
{kind=link}